Adversity is a feature of the life of every child. It can be present when a child is learning a new skill, on their first day of school, when they are negotiating conflicts and when their ambition exceeds their ability. For some children, such as those who have chronic medical conditions and disabilities, adversity is a predominant and pervasive feature of their day-to-day life. Some children demonstrate persistence in the face of adverse conditions, whereas others shy away from them. Whatever the source of adversity, the ability to cope with it is critical to a child’s development and to them experiencing a productive, successful and satisfying life.
Psychological strength, or resilience, is directly implicated in a child’s capacity to cope with adversity. Resilience represents that quality of the individual that enables them to persist in the face of challenges and recover from difficulty or hardship. Resilience strengthens a child and enables them to try new experiences, accept challenges, and cope with frustration and failure. Resilience sustains a child through hardship and supports the realisation of dreams and aspirations. As such, the promotion of resilience is a universal concern of all adults with a caring concern for children.
A child’s capacity to cope with adversity (i.e. their resilience) varies over time in association with biological, psychological and environmental influences, and the interaction of these.
Biological influences include the child’s temperament and their susceptibility to stress and anxiety. Psychological influences include the child’s capacity to develop and maintain constructive beliefs in conditions of adversity, including beliefs about personal worth and competence, expectations of social support and beliefs about the world in which they live. Environmental influences include the extent to which the environment satisfies the needs of the child, including the child’s need for love, acceptance, protection, safety, shelter and physical sustenance.
If you like my previous post regarding a AAA-Approach to overcoming attachment disorders, you can access my article published in the Educational and Child Psychology Special Issue on Attachment in the Publications page of www.securestart.com.au.
Attachment is a term used to describe the dependency relationship an infant develops towards his or her primary caregivers. The development of strong and secure attachments is a critical developmental task of infancy and early childhood. Attachments influence the developing child’s emerging beliefs about themself, others and the world in which they live. Infants become attached to the people who provide physical and emotional care on a continuous and consistent basis. Quality of care and the infant’s early experiences influence the type of attachment the infant develops. When care is grossly deficient and early experiences are characterised by physical and emotional distress, the infant’s attachment to its caregiver is also disturbed. Children who display markedly disturbed and developmentally inappropriate social relatedness in most contexts, and who have experienced grossly deficient care, might accurately be diagnosed with Reactive Attachment Disorder (RAD) or Disinhibited Attachment Disorder (DAD).
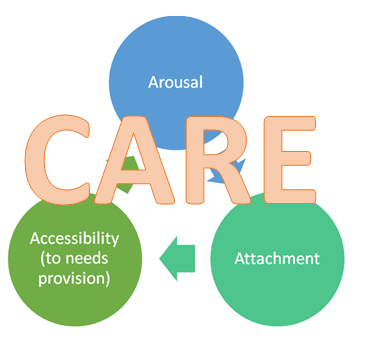
Attachment-disorders arise under conditions where the infant’s caregiver(s) fail to consistently offer experiences of their accessibility to the infant, of their understanding of the infant’s physical and emotional needs and responsiveness to these needs, and of their emotional connectedness to the infant and regulation of the infant’s emotions. Inconsistent regulation of the infant’s experiences of distress, and the infant’s associated high levels of physiological arousal, is particularly detrimental. The outcome is children who think of themselves as unlovable and undeserving, of others as mean and uncaring, and of their world as a harsh place. Their experience of inconsistent caregiver accessibility leaves them excessively preoccupied with influencing their environment in order to access their needs. Their experience of inconsistent emotional connectedness with their caregiver(s) and inconsistent soothing when they are distressed leaves them prone to poorly regulated emotions and behaviours.
Successful management of attachment-disordered children and the remediation of their attachment difficulties begins with enriching their experience of caregiver accessibility, understanding, responsiveness and emotional connectedness. Achieving lower levels of physiological arousal is also critical.
In my first book A Short Introduction to Attachment and Attachment Disorder (JKP, 2009), I share my insights regarding the care and management of attachment-disordered children. In my forthcoming JKP title A Short Introduction to Promoting Resilience in Children, I extend these ideas to the promotion of positive adjustment and resilience, not just among attachment-disordered children, but among all children.
Therapy is more likely to be beneficial when children are willing participants. Many children are reluctant, at-least initially, to attend and be involved in therapy. Either they don’t know what to expect, which causes anxiety, or they think that they have to attend because they have been “bad”. However, almost all children enjoy playing and engaging in fun activities with a lively adult. So, incorporating fun activities into therapy is a good way to help children feel relaxed about attending therapy and, indeed, increases their motivation to attend.
Making and maintaining a connection
Research has shown that the heart rates of mothers and infants parallel each other during play[1]. Heart rate is a sign of the level of activity of the nervous system, which is commonly referred to as arousal. Arousal is the physiological component of emotion. When we experience emotion, arousal changes. So, when the heart rates of mothers and infants mirror each other during play, it is possible to conclude that the adult and child are emotionally-connected to each other.
Emotional-connection, as occurs during play, offers a safe environment for the exploration and expression of a range of emotions and, ultimately, a broad and rich emotional repertoire.
Perhaps, most important of all, emotional connection offers experiences of being heard and acknowledged at an emotional level. Feeling heard and acknowledged in this way offers a powerful form of validation that serves as a ‘psychological innoculation’ against mood disorders and other adverse psychological consequences of invalidation (i.e. the experience of not being heard and understood by others) in adulthood.
Emotional connection and, by extension, play, supports emotional health.
Encouraging self-regulation
Most children who are referred for therapy have trouble controlling their emotions, their behaviour, or both. Emotional-connection, as occurs during play, supports the development of emotional awareness (self and other), which is a precursor for empathy and socio-emotional reciprocity (that is, regulating ones own emotions and behaviours in order to achieve mutually desirable outcomes when interacting with another person). Further, emotional-connectedness, as occurs during play, supports opportunities for co-regulation, whereby the adult assists the child to regulate their emotions. Co-regulation is influential in the development of self-regulation.
In sum, play offers opportunities for supporting emotional awareness, emotional self-regulation, and empathy.
Affirmative Experiences
Children who are referred for therapy hold beliefs about themselves, about others and about the world in which they live. Often, one or more of these areas of belief is negative. That is, they might see themselves as bad and helpless, others as mean and uncaring, and/or the world as a harsh place. Simply telling children that they are good, that others are caring and understanding, and that the world is a safe place is rarely effective in changing children’s beliefs. Rather, they need to experience themselves, others and their social world differently. During therapeutic play, children experience themselves as likeable and capable, experience others as fun and “nice”, and their world as safe and a source of happy experiences. This facilitates trust in others and the perception that therapy is a safe place for conversation about the reasons for their emotional distress and/or behaviours of concern.
Play is an important and natural approach for promoting the emotional wellbeing and positive adjustment of children and young people.
If you like this article, please subscribe to this blog to receive an email notification when other practical ideas and guidance is published.
Join 5,452 other subscribers
You can access more information about my therapeutic parenting programs by clicking the links below:
Disclaimer: While great care is taken to ensure that the advice on this site is widely applicable and based on sound psychological science, it may not suit the individual circumstances of all visitors. If you have any concerns about applicability to your circumstances, please consult a qualified professional near to you.
Join 5,452 other subscribers
Colby Pearce
Search this site
Supporting consistent Therapeutic Caregiving
Companion App for Therapeutic Classrooms and alignment with home.