
Why have Therapeutic Models of Care?
In an online survey of carers of ‘looked-after-children’ (defined as children who do not live with a birth parent(s) and are in a relative or kinship care placement, adoptive placement, foster placement or residential care placement), in which responses were received from 157 carers over a one-week period in September/October 2014, only 16% reported using a known Model of Care to inform their caregiving.
This begs the following question: What do carers rely on to inform their care of these often troubled and challenging children?
Instinct?
Experience?
Advice? (only half of respondents in the carer survey reported that they are supported in the role by a social worker)
Is this a problem?
Well, lets look at some figures for adult outcomes for children raised in out-of-home care:
- Those with 3 or fewer placements were more likely to finish school 1 (65% of children in foster care experienced 7 or more changes in placement 2)
- Three times more likely than the general population to be living in poverty 2
- Up to nine times more likely to become homeless 3
- Five times more likely to have PTSD 4
- Up to ten times less likely to complete a bachelor degree 2
- Sixty-six times more likely to have children needing public care 5
Children in out-of-home care require more than conventional care based on instinct and experience alone.
We need to do better at supporting carers of these vulnerable children with therapeutic approaches to caregiving that are user-friendly, evidence-based and sustainable over time.
The Triple-A Model of Therapeutic Care was developed across almost twenty-five years of my work as an applied researcher and clinician.
There are a number of therapeutic models of care on offer to individuals and organisations who support looked-after-children and those who care for them.
Nearly all are embedded in attachment theory.
Many incorporate emerging knowledge about the effects of trauma in the first care environment on the developing brain (a.k.a. Neurobiology of Trauma).
Triple-A incorporates both.
So, what is its point of difference?
Before I answer, let me return to the results of the carer survey.
Participants in the survey were provided with a list of behaviours commonly observed among children in out-of-home care and have a history of early or developmental trauma (a.k.a. abuse and neglect), as presented under the heading “Manifestations” in the table below taken from Pearce, C. A Short Introduction to Attachment and Attachment Disorder. Jessica Kingsley, London. Participants were asked What behaviours do you typically see in the children in your care that cause you concern?
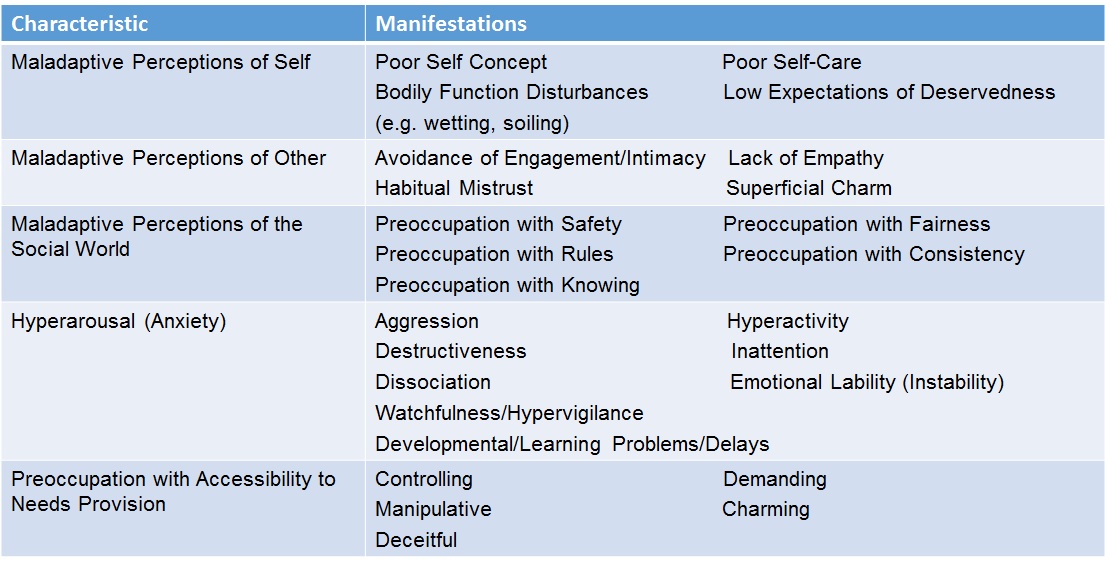
The most commonly reported behaviour concerned children being demanding; that is preoccupied with their needs and controlling the accessibility and responsiveness of their caregiver.

Viewed in terms of the Triple-A Model, the data looks like this:
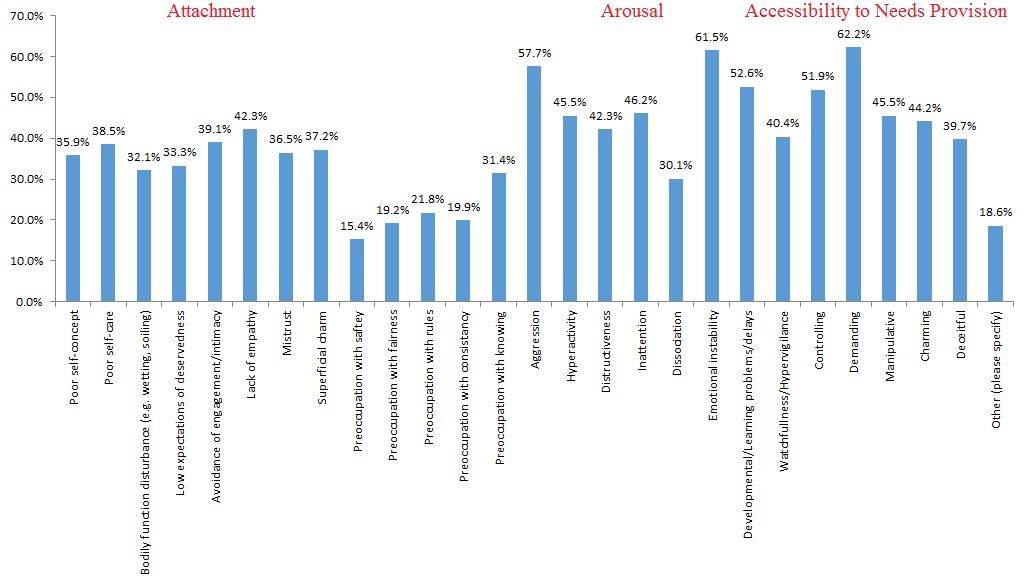
The most commonly reported behaviours that carers of looked-after-children report as causing them concern are under the heading “accessibility to needs provision”. And, yet, other therapeutic models of care do not address this issue directly.
The most significant difference between Triple-A and other therapeutic models of care is that Triple-A draws on the science of human learning to facilitate a better understanding of the looked-after-child’s inordinate preoccupation with their needs and with accessibility to needs provision.
What is Triple-A?
The Triple-A Model of Therapeutic Care is a tripartite model that addresses the impact of abuse and neglect on three key areas of the child’s psychological functioning 6:
- Attachment (science of relationships and social-emotional development)
- Arousal (psycho-physiology of emotion and behaviour activation systems – a.k.a. “Neurobiology of Trauma”)
- Accessibility to needs provision (science of human behaviour).
The Triple-A Model of Therapeutic Care is a step-by-step approach that:
- Offers children experiences that support the promotion of secure attachment, thereby restoring the foundations for a happy and successful life after experienced abuse and neglect.
- Offers children experiences that promote feelings of safety in relationships to reduce anxiety proneness and promote new learning and the development of brain structures responsible for thoughtful consideration, planning and effective action.
- Offers children experiences that facilitate new learning that their needs are understood and important and will be met reliably and predictably through conventional care.
The Triple-A Model of Therapeutic Care is concerned with carer wellbeing and incorporates information and strategies for preventing vicarious trauma (a.k.a. compassion fatigue) among carers of children recovering from abuse and neglect.
The Triple-A Model of Therapeutic Care incorporates a built-in evaluation methodology. Ongoing evaluation shows that implementation of the Triple-A Model of Therapeutic Care results in targeted changes in caregiving behaviour. Children to whom the Triple-A Model of Therapeutic Care is delivered show evidence of:
- Improved attachment security (they increase their independent play, reflecting an emergent secure base);
- Reduced arousal (they sleep better, they waken happier, they have fewer emotional outbursts and their outbursts are of shorter duration); and
- Reduced preoccupation with their needs (they are less demanding/coercive/ preoccupied with needs/wishes).
The Triple-A Model of Therapeutic Care© can be delivered to alternate care programs internationally and has been the preferred therapeutic model for TUSLA foster carers in Donegal, Ireland since January 2016.
For more information about Triple-A, contact the author, Colby Pearce, at colby@securestart.com.au
If you found the content of this article interesting and/or useful, please share it using the sharing buttons below.
Please subscribe to this blog to receive further articles when they become available. Click “Follow” in the side bar.
You can access more information about my programs by clicking the links below:
 Triple-A Model of Therapeutic Care
Triple-A Model of Therapeutic Care
The CARE Therapeutic Framework
Helping Children and Young People Realise their Potential
Another place way to connect with my work is to follow one or more of my pages on Facebook:
To Connect with me on LinkedIn or Twitter click below:
References
1.Cashmore, J.A. & Paxman, M. (1996). Wards Leaving Care: A Longitudinal Study. Sydney: Department of Community Services
2.Pecora et. al. (2010) Rates of mental, emotional and behavioural disorders among alumni of family foster care ibn the United States: The Casey National Study. In E Fernandez & R. Barth (Eds) How does foster care work? International evidence on outcomes. (pp, 166-186)
3.Casey Family Programs (2001) It’s my life: A framework for you transitioning from foster care to successful adulthood. Casey Family Programs: Seattle
4.Pecora, P.J. (2010). Why current and former recipients of foster care need high quality mental health services. Administration and Policy in Mental Health and Mental Health Services Research. (37(102), 185-190
5.Jackson, S & McPharlin, P. (2006). The education of children in care. The Psychologist, 19(2): 90-93
6.Pearce, C.M. (2010). An Integration of Theory, Science and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children – A Triple A Approach. Educational and Child Psychology (Special Issue on Attachment), 27 (3): 73-86











Reblogged this on The Family of 5's Journey and commented:
I have read some of Colbys books and highly recommend them, his latest blog highlights the importance of ‘Foster/Adoptive/Kinship parents being supported throughout their therapeutic parenting journeys, something we here in the UK need to get better at. The support provided to adopters here generally stops once the adoption order is granted, or if your lucky 3 years after the order is grated. Therapeutic parenting of a traumatised child is a life long commitment and thus needs, life long support. These traumatised children deserve better outcomes, not worse.
Hello. Thanks for sharing this on your blog thefamilyof5. I hope it generates some interest in your network in my work and in Triple-A. We are soon beginning implementation in Ireland and hope to have some projects in the UK very soon. Best wishes. Colby