
Complex Trauma occurs when children experience prolonged and debilitating fear and distress as a result of adverse experiences that occur recurrently and/or in combination, and where the person or person’s who are responsible for keeping the child safe from harm and alleviate their distress is/are:
- unable to alleviate the child’s distress, or . . .
- are responsible for the child’s fear and distress.
The type of trauma being referred to here is also known as:
- Complex Developmental Trauma – because it occurs during a period of formative development and shapes all aspects of the child’s development;
- Attachment Trauma – because it usually occurs in the context of the child’s first attachment relationships, where one or other or both of the child’s first attachment figure(s) is responsible for the trauma experience;
- Abuse – an act of commission that results in physical and/or emotional and/or psychological harm; or
- Neglect – an act of omission that results in physical and/or emotional and/or psychological harm.
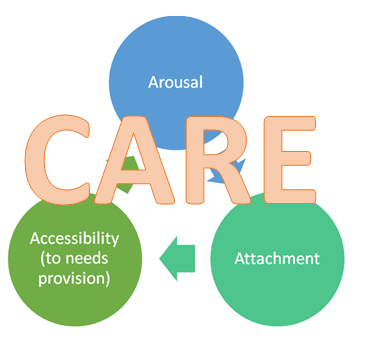
Complex trauma adversely impacts three key factors that play an important role in the developing child’s approach to life, learning/development, and relationships:
- Attachment (or, how the child thinks about, and interacts with, themselves, others and their world);
- Arousal (or, the psycho-physiology of performance, emotion and behaviour activation systems);
- Accessibility to needs provision (or, what the child has learnt about the accessibility and responsiveness of adults in a caregiving or caretaking role).
Attachment refers to the dependency relationship an infant develops to his or her primary caregivers during the first years of life. Our knowledge of attachment derives from Attachment Theory. Attachment Theory was initially developed in the 1940’s, in part to account for observations that were being made of institutionalised children and those who experienced prolonged separation from their primary caregivers; including by reason of lengthy hospital admissions and those children displaced from their families during World War II (Bretherton, 1992) .
Since its early development, Attachment Theory has been the focus of an enormous amount of research and has become widely used in child protection as it offers an explanatory framework for differential outcomes for children based on caregiving practices. In addition, Attachment Theory informs us about a child’s relationship with themselves, others and their world.
Arousal refers to the level of activation of the nervous system. From a psychological point of view, arousal is significant for (at-least) three reasons. Firstly, arousal affects how well we perform tasks, and activities more generally. Secondly, arousal is implicated in how we feel. Thirdly, arousal is implicated in how we behave, including our approach to life and relationships. In particular, arousal is implicated in the behaviour activation system that is activated when individuals perceive a threat to themselves or someone close to or close by them and their associated feeling of anxiety (known as the fight-flight-freeze response).
Accessibility to needs provision refers to what children have learnt about the reliability and predictability with which their needs will be addressed by adults in a caregiving role, and learnt behaviours that serve to reassure the child that their needs will be satisfied. Accessibility to needs provision is based on Learning Theory and the Operant Conditioning paradigm (Ferster & Skinner, 1957; Skinner, 1938).
In combination, I refer to these three factors as the “Triple-A Model”; or “Triple-A” for short (Pearce, 2010).
In the resources below I provide additional detail about how complex trauma impacts attachment, arousal and what the child learns (and learns to do) about accessibility to needs provision. Thereafter, I a set-out a series of practical, user-friendly strategies for addressing these aspects of the child who has experienced complex trauma following the CARE Model (Pearce, 2016):
- Consistency
- Accessibility
- Responsiveness
- Emotional Connectedness
I do hope that you decide to access these complementary resources or supporting consistency o therapeutic care and management across home and school for children who have had a tough start to life.
Get a free introduction to the resources here!
For individual purchasers – Carer Resource
Buy now and we will email your personalised copy of the resource (Please allow up to 2 business days for us to respond to your payment).
A$16.50
For more information, or for organisational purchasers, click here.
For individual purchasers – School Resource
Buy now and we will email your personalised copy of the resource (Please allow up to 2 business days for us to respond to your payment).
A$16.50
For more information, or for schools/organisational purchasers, click here.


References
Bretherton, I. (1992). The Origins of Attachment Theory: John Bowlby and Mary Ainsworth. Developmental Psychology, 28: 759-775.
Ferster, C.B. and Skinner, B.F. (1957) Schedules of Reinforcement. New York: Appleton-Century-Crofts
Pearce, C. (2016). A Short Introduction to Attachment and Attachment Disorder (Second Edition). London: Jessica Kingsley Publishers
[Pearce, C.M. (2010) An Integration of Theory, Science, and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children: A Triple-A Approach. Educational and Child Psychology (Special Issue on Attachment), 27 (3): 73-86
[Skinner, B. F. (1938) The Behaviour of Organisms: An Experimental Analysis. New York: Appleton-Century










