Conventional responses to behaviours of concern, such as reward and punishment strategies, are widely considered to be ineffective in addressing the complex and challenging behaviours exhibited by children and young people who have experienced complex, relational, or early/developmental trauma. This is because a number of the preconditions for reward and punishment strategies to work do not exist among these children.
For example, in order for rewards to work, the child or young people needs to believe, based on prior learning, that you will follow through with the promised reward if they exhibit desired behaviour (or inhibit undesirable behaviour). Children and young people who have experienced grossly inadequate care find it hard to trust that adults will follow through with their promises. Rather, they expect to be let-down and are not motivated to work to achieve a reward, instead believing that that they are unlikely to be successful and you won’t follow through anyway.
Further, children and young people who have experienced abuse and neglect view punishments as further evidence of their inherent badness and of the meanness of adults. Rather than being motivated to comply with behavioural expectations to avoid punishment and maintain positive relatedness, they strongly hold on to their beliefs that they are inherently bad and unlovable and that adults are mean and uncaring. They persist in their behaviour of concern because it satisfies a need, including the need to feel like they can influence what happens in their world. They do so without consideration of the impact of their behaviour on their relationships with others, because they don’t expect to have good relationships, especially with adults in a care and management role, anyway.
Responding to behaviours of concern exhibited by these children and young people requires a different approach. It requires us to acknowledge and accept that all behaviour occurs for a reason. If it did not achieve a desired outcome when it was first exhibited and at-least sometimes thereafter, it would have been dropped in favour of a more successful behaviour. It then requires us to consider what the reason for the behaviour is and respond to that in a way and until the behaviour stops or is exhibited at more normalised frequency, intensity, and duration. This is the therapeutic response to complex and challenging behaviours exhibited by children and young people who are recovering from a tough start to life.
The decision to remove a child or young person from the care of their birth parents is a grave one that confronts child protection authorities daily. Removal occurs with the intention of protecting the child from harm and securing their safety. The wider community expects child protection authorities to intervene to protect children from harmful circumstances and secure their care and protection. Indeed, child protection authorities are often subject to intense media scrutiny and community outrage in circumstances where they are perceived to have not intervened to protect a child, and the resultant harm becomes known to the community.
There is positive intent in removal. But what are the negative impacts, if any, of this well-intentioned action to secure a child’s safety and protection from harm?
An intriguing group of children are those who are removed from the care of their biological parents at or very close to birth, and who remain in care long-term. Carers of these children are often perplexed when, years later, and notwithstanding loving care afforded to them, the children show many of the same complex and challenging behaviours commonly observed among children who have experienced abuse and/or neglect prior to their removal. This has led to consideration of the impact of pre-natal trauma on the developing child. However, my experience has taught me that there is another valid line of enquiry into why children removed at or close to birth exhibit maladjustment not dissimilar to those who are removed later, and which provides an insight into the potential negative impact of removal more generally.
Irrespective of when they are removed from the care of their birth parents, children who remain in out-of-home care appear to suffer from difficulties in the areas of self-worth, identity, and belongingness which, in turn, result in complex and challenging relational behaviour. When they are old enough to do so, these children and young people speak of a profound loss associated with not having had the opportunity to be raised within their birth family. They question their worth in relation to this. Why could their birth parents/family not make more of an effort? Didn’t they love me? Am I unlovable?are common insecurities. Who am I? and Where do I belong? are others.
As they seek answers to these questions through behaviours that are experienced by their caregivers at home, in school, and in other domains of their life as perplexing and challenging, these questions crystallise into an enduring sensitivity about self-worth, identity, belongingness, and relational connection. In turn, this sensitivity manifests in:
self-defeating behaviours (such as precocious experimentation with drugs and alcohol, precocious sexual activity, and suicide and self-harm)
disturbed relational behaviour (such as coercion, rejection, instability)
identity concerns (such as gender dysphoria and sexuality concerns)
Too often, the reaction of well-meaning adults to these aspects of the child or young person’s approach to life and relationships only confirms and reinforces their fear that they are worthless and unlovable, and maintains maladaptive behaviour and identity concerns.
So, what is the answer?
My experience has taught me that we engage with and support these children and young people in ways that promote their self-worth and belongingness as a vital priority. Unfortunately, this can be a ‘double-edged sword’ as the more they are loved the more disappointed they feel about those who they perceive did not (or do not) love them enough; potentially compounding the issue.
In addition to engaging with these children and young people in ways that support their worthiness, identity, and belongingness, there needs to be greater recognition of the enduring role and importance of birth parents and family after removal. There needs to be greater recognition of the negative effects of removal, which present asan enduring sensitivity about worth, identity, belongingness, and connection to others.
Removing children often results in a worsening of the pre-existing maladjustment of birth parents as their own worth is eroded by the removal and associated reasons for it. Where it is possible and safe to do so, child protection authorities need to meaningfully engage birth parents in recognition of their enduring role and importance in the life of the child, and support the maintenance of best connections between the children and their birth parents/family.
As John Bowlby once wrote: If we value our children we must cherish their parents.
It is not anticipated that this is or will be easy. Community sentiment, echoed in the media, often asserts that child protection authorities need to remove all children at risk and give them the opportunity to grow up in a place of safety. My experience has taught me that support of an enduring connection with birth parents/family represents the best chance of meeting community expectations about outcomes for children and young people in need of protection and care.
In this the final blog of the series, I will present what I think functional learning about the accessibility and responsiveness of adults in a caregiving role for needs provision looks like. I recommend that the reader also take a look at the previous blog posts in this series, which can be accessed below:
Children and young people who are recovering from a tough start to life often present in a manner that reflects that they are unsure about, or don’t trust, that adults in a caregiving role will be accessible to them, understand their needs (and reasonable wishes), and respond to them in a consistent and predictable manner. This manifests in inordinately demanding behaviour, of caregiver proximity and responsiveness, and/or inordinate self-reliance. Sometimes, they alternate between the two. Their caregivers typically feel overwhelmed and frustrated which, in turn, often leads to withdrawal, restriction, and further unresponsiveness; the impact of which is worsening of the child or young person’s preoccupation with accessibility to needs provision.
This problem behaviour arises because of what the child learns about the accessibility and responsiveness of adults in a caregiving role during the early developmental period where caregiving is inconsistent and inadequate. These children and young people typically learn that you cannot always rely on adults in a caregiving role when their care was adversely impacted by addiction, mental health difficulties, relationship issues, and poor parenting knowledge.
]
Children and young people who are recovering from a tough start to life benefit from care that supports new learning that adults in a caregiving role can be relied upon to be accessible and responsive to them. To learn more about caregiving strategies to achieve this I refer the reader to A Short Introduction to Attachment and Attachment Disorder (Second Edition).
Evidence that the children are making this new learning includes acceptance of proffered care, exploration of their world, being able to share with others, age-appropriate dependency, acceptance of temporary separations, independent play, and age-appropriate independence, including with self-care routines.
I cannot underestimate the importance of knowing what success on behalf of children and young people in our care who are recovering from a tough start to life looks like, and have included below and table for quick reference based on the Triple-A Model (Pearce, 2016, 2012, 2011, 2010).
Arousal
Attachment
Accessibility (to needs provision)
Calmness
Giving things a go
Accepting separations
Restful sleep
Confident exploration
Sharing
A range of natural emotion
Joining in
Seeking help when needed
Easily soothed
(Appropriate) Independence
Independent play
Cooperation
Accepting Challenges
Exploration
Sustained attention (focus)
Seeking help when needed
Feeding self
Bladder and bowel control
Having fun
Independence
Attaining milestones
Making friends
Academic success
Accepting Challenges
Grooming
Using words to communicate
Positive self-esteem
If you enjoyed this series and would like to write about topics related to child protection, therapeutic care, and psychology service provision, do get in touch.
References:
Pearce, C.M. (2016) A Short Introduction to Attachment and Attachment Disorder (Second Edition). London, Jessica Kingsley Publishers
Pearce, C.M (2012). Repairing Attachments. BACP Children and Young People, December, 28-32
Pearce, C.M. (2011). A Short Introduction to Promoting Resilience in Children. London, Jessica Kingsley Publishers
Pearce, C.M. (2010). An Integration of Theory, Science and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children – A Triple A Approach. Educational andChild Psychology (Special Issue on Attachment), 27 (3): 73-86
Pearce, C.M. (2009) A Short Introduction to Attachment and Attachment Disorder. London, Jessica Kingsley Publishers
In this, the third blog in this series, I will write about what a well-modulated nervous system looks like among children and young people who are recovering from a tough start to life. Please also refer to the first and second blogs in this series, which can be accessed here and here.
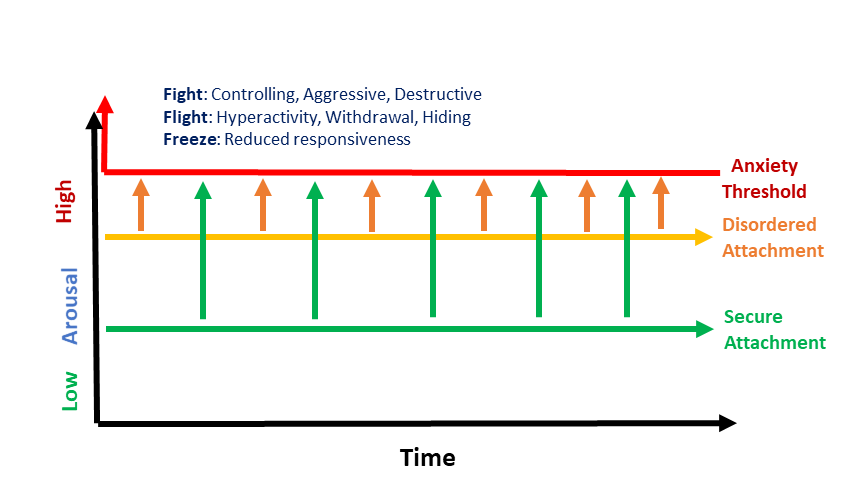
Children and young people who are recovering from a tough start to life typically exhibit behaviours associated with an over-activated nervous system, or hyper-arousal. This can manifest in difficulty sleeping, emotional reactivity, and motor restlessness. Coupled with their proneness to approaching life under the influence of negative beliefs about self, other, and world (AKA attachment representations, or internal working models – refer to the second blog in this series) these children and young people are prone to anxiety and behaviours associated with the fight, flight, freeze response, including:
controlling, aggressive, and destructive behaviours (fight),
hyperactivity, running and hiding (flight), and
reduced responsiveness (freeze).
Unfortunately, these behaviours are not always understood to be non-volitional responses to activation of the nervous system’s in-built survival response. Rather, they are often seen simply as bad behaviour, and responded to with anger and disapproval. This only serves to further heighten arousal and confirm the child or young person’s belief that they are bad and unsafe and that others are threatening, leaving them even more prone to future anxiety and behaviours associated with the fight flight freeze response.
We are very good at noticing these signs of a nervous system under stress or duress; albeit that we don’t always see it for what it really is. Harking back to the first article in this series, we are comparatively less likely to recognise evidence of a well-modulated nervous system. If we are not looking for evidence of a well-regulated nervous system, we are likely to miss signs of it, with the result that we continue to notice and respond disproportionately to so-called problem behaviour, to the detriment of the child’s emerging self-image and our own feelings of competency in a care and management role.
So, what does a well-modulated nervous system look like? Children and young people who have a well-modulated nervous system experience longer periods of wellbeing and a range of natural emotions that are congruent with context and [easily] self- or co-regulated (that is, able to be regulated with the assistance of an attuned adult). They perform better in learning tasks and other tasks of daily living. Their developmental progress is within normal limits, or near to. They explore their world, including relationships, unhindered by anxiety. They sleep well and have less sensory issues. They are accepting of adult authority, and comparatively easy to get along with.
So, look for the signs of a well-modulated nervous system. You are more likely to feel optimistic about the future of the child or young person. They will, in turn, feel more positive about themselves.
In the first blog of this series about child welfare intervention outcomes, I wrote about the importance of knowing, and being able to say, what progress toward successful outcomes looks like. In this second blog of the series, I will talk about what attachment security looks like.
Before I get into it, I want to make the point that I am not talking about the reduction in a behaviour or behaviours of concern, or symptom reduction. This is still ‘problem-focused’, with the same associated difficulties as I highlighted in the first blog. Rather, I am taking about what progress towards recovery looks like for children and young people who are recovering from a tough start to life.
In the first blog in this series I referred to the Triple-A Model (Pearce, 2016, 2012, 2011, 2010), which I use as an explanatory framework for understanding the impact of early relational trauma on the developing person. The Triple-A Model refers to Attachment, Arousal, and Accessibility to Needs Provision. These constructs also help us to reflect about and identify what progress towards recovery from early relational trauma looks like. In this article I am going to refer to the first construct, attachment, and what progress towards attachment security looks like.
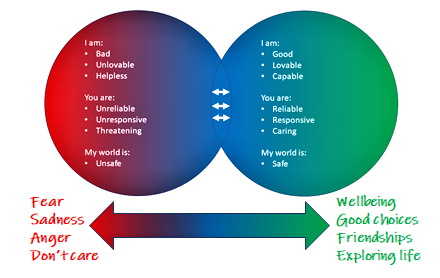
Early relational trauma negatively impacts attachment security in the developing child and, in turn, their approach to life and relationships. This is, perhaps, best represented in the internal working models, or attachment representations, that develop in the context of our early attachment experiences. These take the form of beliefs that, mostly subconsciously, influence our approach to life and relationships. They are the beliefs that are held about ourselves, others, and the world in which we live.
Among children and young people who have experienced early relational trauma, the attachment representations that influence their approach to life and relationships are predominantly negative. They believe themselves to be bad, unlovable, unworthy and incompetent; they believe adults in a caregiving role to be unresponsive, uncaring, and unsafe; and they believe that the world in which they live is a harsh and dangerous place. They approach life and relationships under the influence of these beliefs, and this is reflected in their behaviour. That is, their behaviour reflects their inner world and the beliefs they hold about themselves, others, and their world.
In contrast, children who were raised in safe and nurturing homes predominantly approach life and relationships under the influence of secure attachment representations. They believe themselves to be good, worthy and capable; adults in a caregiving role to be accessible, responsive, and safe; and they believe their world to be safe and full of opportunities. Their behaviour is largely consistent with these beliefs.
In consideration of the above, when intervening to promote recovery from early relational trauma, we need to turn our mind to what needs to happen to strengthen the influence of secure attachment representations over the young person’s approach to life and relationships. As their behaviour reflects their inner world and attachment beliefs, we need to know what behaviour that is under the influence of secure attachment representations looks like.
In my work with children recovering from a tough start to life, the first thing I look for is that they are making some effort in relation to their appearance. Self-care reflects self care. I also look for natural interest in engagement with me and comfort in separating from primary caregivers. I look for positive and realistic self-appraisals and acceptance of praise. I look for awareness of the experience of others and regulation in consideration of others. I look for a transition from behavioural expression to verbal expression about their needs and experiences. I look for preparedness to try new things and tolerance of frustration and failure. I look for emerging interests and participation in related pursuits. I look for persistence in their endeavours born out of a natural desire to be successful. I look for interactions with me that reflect my role and endeavours with them. I look for choices and actions that reflect a positive sense of their worth. I look for anticipation of a career, of enduring relationships, and of a family of their own.
In addition, I am keen to hear about the following aspects of the child’s approach to life and relationships, and I encourage adults who care for or have a caring concern for these children and young people to look for them too:
Care about appearance
Realistic self-image
Consideration of others
Giving things a go
Confident exploration
Joining in
(Appropriate) independence
Readily soothed or comforted by adult caregivers
Seeking help when needed
Having fun
Making friends
Accepting challenges
Using words to communicate
Empathy
Hopefulness
Dreams and aspirations
Standing up for themself
There are other signs of progress towards recovery from early relational trauma, but these also reflect well-modulated arousal and functional learning about accessibility to needs provision, so I will include these in the next two articles in this series.
Pearce, C.M. (2016) A Short Introduction to Attachment and Attachment Disorder (Second Edition). London, Jessica Kingsley Publishers
Pearce, C.M (2012). Repairing Attachments. BACP Children and Young People, December, 28-32
Pearce, C.M. (2011). A Short Introduction to Promoting Resilience in Children. London, Jessica Kingsley Publishers
Pearce, C.M. (2010). An Integration of Theory, Science and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children – A Triple A Approach. Educational andChild Psychology (Special Issue on Attachment), 27 (3): 73-86
Pearce, C.M. (2009) A Short Introduction to Attachment and Attachment Disorder. London, Jessica Kingsley Publishers
Some know that while attaining my post-graduate qualifications in Psychology I worked for five years as a Research Officer in the local Child and Adolescent Mental Health Service (CAMHS). During this period I worked closely with Psychiatry staff who were both expert practitioners and avid scientists. Looking back, I believe more and more in the importance of expert practitioner’s also conducting research in their areas of practice expertise. Who better to lead research into a field of endeavour than expert practitioners in that space?
I then look at where my own career has taken me, in the field of child welfare. My experience has been that there has not ever been time or allowance to conduct research into the field of endeavour in which I (and many others like me) have built significant expertise through practice. Rather, much of the research that we rely on comes from the academics with a special interest in our area of endeavour.
This is more and more concerning to me, especially in an era where evidence-based practice is the “gold standard”. Where does that leave expert practice built upon years of endeavour working directly with children, young people, and all who play a role in the domains of their lives? What status is accorded to practice expertise? Compared to that which comes out of a university study, I would say less status.
Ideally, expert practitioners in the field of child welfare would have time and allowance to be involved in research into best practice and practice knowledge. There is no substitute for conducting the assessment, making the recommendations, implementing the treatment plan, and reviewing the outcomes across one, or two, or more decades of practice, I believe.
Child welfare leaders and academics with a special interest in knowledge and practice in child welfare, it is time to engage practice leaders in research in child protection and child welfare.
(Please note that my reflection is largely based on my observations and experience in the jurisdictions in which I have worked. If the situation is different elsewhere, I would greatly appreciate hearing from you!)
What outcomes do you expect to see as a result of my service provision?
This is a question I routinely ask in my work. Put another way:
What are the benefits the individual(s) or organisation who engages my services anticipate that they will see and experience?
What will success in our joint endeavours look like?
How will you know that my involvement has made a positive difference?
These are, perhaps, the fundamental questions that get at the hopes of the engaging entity.
Yet, I have found that these are some of the most difficult questions for the engaging entity, be that a parent or other caregiver, a representative of a school, or a representative of child welfare organisation, to answer.
In straightforward terms, it has been my experience that engaging entities find it very difficult to express what successful outcomes look like.
Why might this be the case? The answer lies, in part, in what we typically attend to as we negotiate our lives and our roles.
Humans are, first and foremost, problem solvers. Problem solving has allowed us to successfully negotiate a myriad of challenges and successfully adapt to our living conditions through history and in our contemporary world. As an illustration of this, when I show the image below during training or supervision, and ask my audience what is the first thing they notice, they almost invariable identify the simple maths equation that is incorrect, in the bottom left corner. No-one, and I have been using this graphic for several years, has ever said that nine of the equations are correct.
No-one has ever said that nine of the equations are correct.
We instinctively notice problems and are very good at saying what they are. We are also very successful, as a species, in solving them, However, in my experience working in child welfare and psychology service provision in this field, where problems abound, there is a manifest difficulty in being able to say what a good outcome of an intervention or process looks like.
The danger here lies in missing the evidence of success in our endeavours. Why? Because child welfare work can be overwhelming. If we miss the evidence of our successes and focus selectively on problems to solve, we are vulnerable to feeling like a failure in our role, and give up. Further, as children and young people see themselves as they experience others to see them, our selective focus on problems results in them seeing themselves as a problem.
Even in writing this article I am guilty of the same selective attention to problems; in that the inordinate focus on problems is a problem!
We need to get better at knowing what success in our endeavours looks like; in responding to the questions posed at the beginning of this article. The knowing supports thinking which, in turn, supports noticing. The noticing supports self-efficacy and identification of effective interventions. Noticing progress and success supports a healthy self-image among children and young people who are recovering from a tough start to life.
During the Kinship CARE Project, which ran from 2018 to 2020 as a training initiative of Secure Start with support from the Department for Child Protection, South Australia, we collected data about a range of outcomes, from attendance data to satisfaction with the training and the like. However, perhaps the most heartening data was the proportion of participant kinship carers who reported feeling more confident in the role as a result of their participation in the Project.
Similarly, in the implementation of the Triple-A Model of Therapeutic Care in the TUSLA Fostering Service in Donegal, Ireland (soon to enter its eighth year of continuous implementation), the most heartening outcome is the longevity of the implementation, the sustained interest of local general and relative foster carers, and the extension to the implementation of a complementary training program in local schools over the last 18 months.
(Pearce, 2009, 2010, 2011, 2012, 2016)
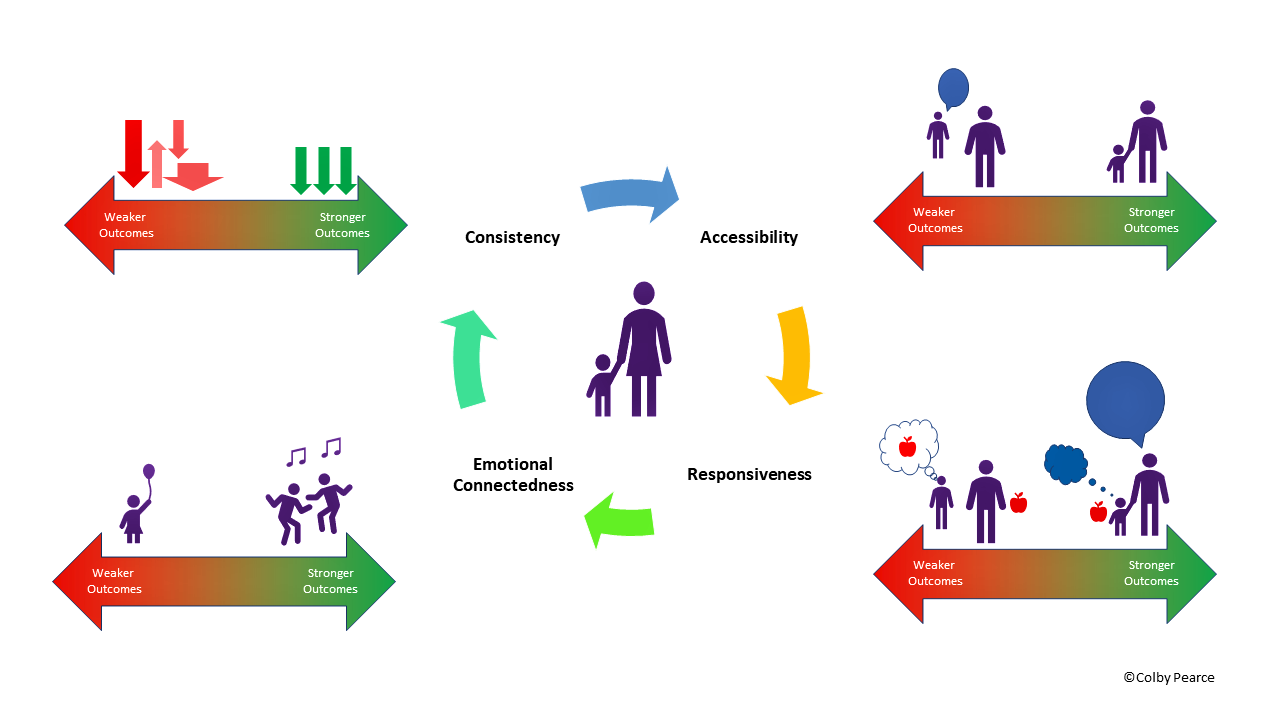
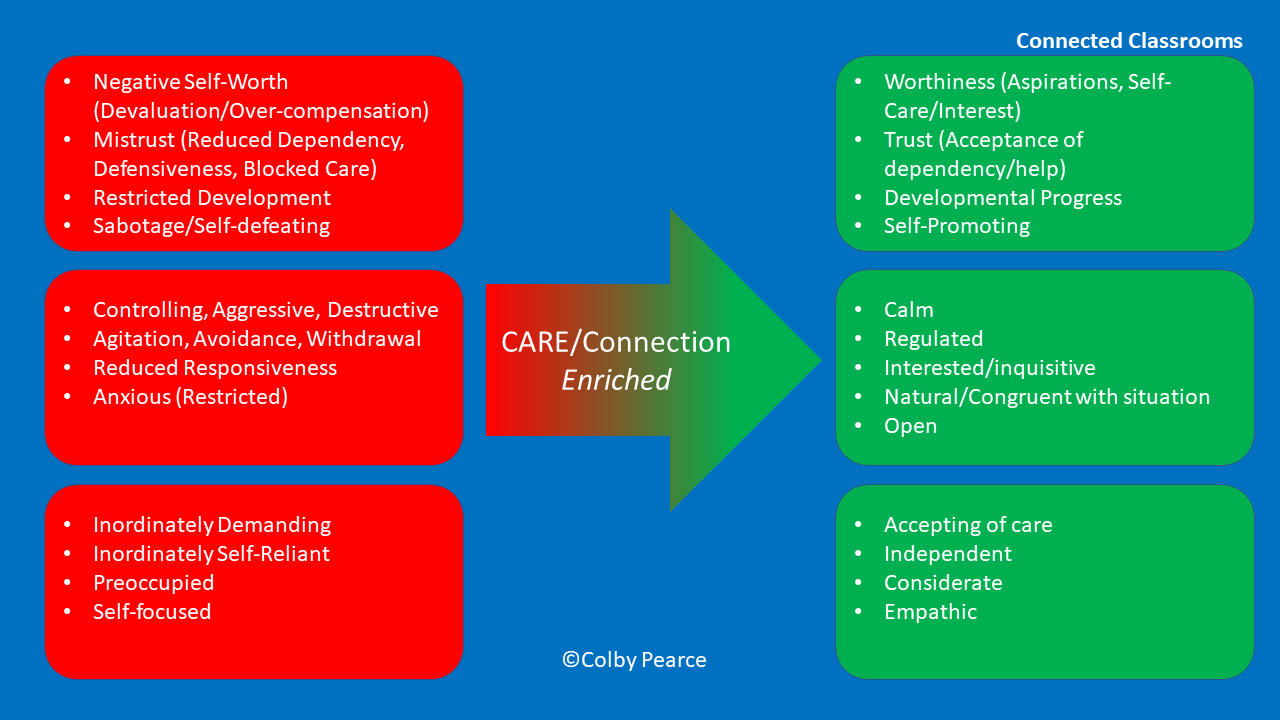
In my clinical work with children and young people who are recovering from a tough start to life I reflect particularly on the Triple-A Model and what positive outcomes in terms of attachment security, arousal modulation, and functional new learning about accessibility to needs provision look like, as reflected in the graphic below which is drawn from a number of my programmes:
In the next article in this series I will write about more what a secure attachment style looks like and, thereafter, about what a well-modulated nervous system looks like and what functional learning about access to needs provision looks like.
References:
Pearce, C.M. (2016) A Short Introduction to Attachment and Attachment Disorder (Second Edition). London, Jessica Kingsley Publishers
Pearce, C.M (2012). Repairing Attachments. BACP Children and Young People, December, 28-32
Pearce, C.M. (2011). A Short Introduction to Promoting Resilience in Children. London, Jessica Kingsley Publishers
Pearce, C.M. (2010). An Integration of Theory, Science and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children – A Triple A Approach. Educational andChild Psychology (Special Issue on Attachment), 27 (3): 73-86
Pearce, C.M. (2009) A Short Introduction to Attachment and Attachment Disorder. London, Jessica Kingsley Publishers
A child leaves their placement to attend school, where acceptance and belonging are contingent on adhering to the school’s behaviour expectations. They leave school to go to sports practice, where acceptance and belonging are contingent on being good enough to make the team. The child returns to their placement, where acceptance and belonging are contingent on the model of care being effective. The child leaves school early the following day to attend family contact, where acceptance and belonging are contingent on their parent being able to set aside their enmity towards child welfare authorities in order to focus their attention and love on the child. The child attends psychotherapy, where the therapist attempts to communicate a big enough dose of acknowledgement and care to compensate for all of the inconsistencies in the child’s life and support a strong and healing sense of self-worth. The child leaves care ….
Time to break down the silos and integrate a holistic approach in all of the domains of a child’s life.
I recently wrote about five areas of activity in a child’s life that together play key roles in achieving positive outcomes for children and young people in out-of-home care (read here). These five areas of activity involve contributions from child protection staff, school staff, foster, kinship, and residential carers (and their support agencies), therapists working with the child, and the broader community. Given the number of players involved, how important is it that they are aligned in their approach to the care of the child or young person in out-of-home care? Is it OK for them all to doing their own thing?
Is it OK for everyone to be doing their own thing?
No matter which position you take with respect to practice alignment, I think we can all agree that the child’s experience is the paramount consideration. It is broadly accepted that children ‘need’ consistency. In my own work, I talk about inconsistency being the ‘primary trigger’. We must be careful to not perpetuate that which bears resemblance to the inconsistencies that pervade a child’s experience in the home deemed unfit for their care and protection.
In my experience, children and young people will be triggered by inconsistencies in their care and management, no matter how well-intentioned. Practice misalignment is a very real threat to achieving best outcomes for children and young people who are recovering from a tough start to life.
So, what is the answer? There are comprehensive endeavours out there that support a common understanding and approach among the adults that care for the child across the domains of their life. Dan Hughes was one of my earliest influences and his PACE and DDP curriculums represent an opportunity to achieve the practice alignment children and young people recovering from a tough start to life need. My own work offers practical knowledge and approaches to care and management that bridge home, school, child protection, community, and consultation room.
Is it time to deliver aligned practice to children and young people recovering from a tough start to life across areas of activity and domains of their life? I think it is past time.
Twenty-seven years continuous work in child protection and child welfare, including ongoing work with young adults who have transitioned from Care, has taught me some extremely valuable lessons about long-term outcomes of a childhood spent in State Care. In particular, it has taught me the importance of five factors that do not always get the attention that is needed when care and protection systems are stretched. In this brief article I will present the five key factors that I think are particularly important for best short- and long-term outcomes for children in State Care, and encourage reflection about what needs to happen when one or more of these five factors are absent. In a nutshell, the content of this article can be summarised in the graphic below:
Best connection with birth parents/family and culture
This first factor is particularly important for a young persons identify, self-worth, and belongingness. Where it is safe to do so, children and young people in State Care benefit from endeavours to promote best connection with their birth parents and/or family, and in the case of indigenous children and young people in particular, their culture (/country and community). Good quality family contact with birth parents and kin supports attachment repair, which is so important to an individual’s overall attachment style and approach to life and relationships. For indigenous children and young people, connection to culture, community, and country counters the negative impacts of systemic racism and supports the worth of their cultural identity.
Stable, Therapeutic Care
It should be a given, but children and young people in State Care do not always receive “Therapeutic Care”. In many jurisdictions, a distinction is made between ‘general’ care and ‘specialist’ or ‘therapeutic’ care. In consideration of the known impacts of maltreatment, separation, and loss, all children and young people in State Care should receive therapeutic care; where therapeutic care incorporates a shared understanding of the impacts of maltreatment, separation, and loss on the developing person, and caregiving measures that mitigate these impacts. I have written extensively in this blog, in periodical articles, and my books about what constitutes trauma-informed, therapeutic care, but it is best encapsulated by the following statement and graphic:
Trauma-informed care is less about developing strategies to address behaviours of concern, and more about responding to the reasons for them.
Trauma informed school
Children and young people in State Care experience further harm when there is misalignment in their care and management between home and school. The harm arises due to the uncertainty this causes for the child or young person about how they will be treated. A common example is the reaction of children and young people in State Care to substitute teachers (aka ‘relief’ teachers). Having experienced maltreatment, separation, and loss, these children and young people crave order. Where there is inconsistency, coercive controlling and testing behaviours represent the child or young person’s endeavours to create order and a sense of predictability, and resolve uncertainty about how they will be treated. Unfortunately for the child or young person, their coercively controlling and testing behaviours are rarely seen for what they are, and negative attributions about self, other, and world are strengthened (thereby necessitating further coercively controlling behaviour to feel safe) when adults respond to the behaviour, as opposed to the reason for the behaviour.
Children and young people in State Care benefit from consistent, trauma-informed care across the domains of their life. This is as true of school as it is the placement, as children and young people (ideally) spend much time at school, and educational participation and attainment is a known predictor of adult outcomes for care-experienced adults.
Community activities and engagement that supports many positive relationships
Attachment theory allows that children and young people form multiple attachment relationships during their formative years. Attachment theory also allows that children and young people form different attachment relationships towards different people, depending on their experience of care from the person. Attachment relationships are formed towards adults who have continuity and consistency in the child’s life, and provide care to them. The child or young person’s overall attachment style is contributed to by all of the significant relationships they form during their formative years. Where some attachment relationships are left unrepaired, the influence of these is buffered by positive attachment experiences; the more, the better.
Trauma-informed therapy
The final factor is access to an experienced therapist who practices in a trauma-informed manner. Ideally, the therapist delivers therapy that supports a secure attachment style, arousal modulation, and functional learning about access to needs provision. The therapist is also a resource for the care team of adults that support the child or young person, including at home and school, in the pursuit of alignment in care experiences across the domains of the child or young person’s life. I have written much about trauma-informed therapy, including in A Short Introduction to Attachment and Attachment Disorder.
Outcomes
In my experience, when all of these factors are in place, children and young people in State Care have the best chance of achieving positive outcomes, including:
•Education attainment
•Aspirations
•Relational connections
•Self-worth
•Wellbeing
•Community Participation
•Identity & Belongingness.
Key Reflections
Where one or more of these factors are not in place, how do you think this will impact outcomes for the child or young person in State Care?
What needs to occur to compensate for the absence of this/these factors?
References
Pearce, C.M. (2016) A Short Introduction to Attachment and Attachment Disorder (Second Edition). London, Jessica Kingsley Publishers
Pearce, C.M (2012). Repairing Attachments. BACP Children and Young People, December, 28-32
Pearce, C.M. (2010). An Integration of Theory, Science and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children – A Triple A Approach. Educational andChild Psychology (Special Issue on Attachment), 27 (3): 73-86
Available research, and anecdotal experience, suggests that children and young people who foster play a critical role in the success, or otherwise, of an out-of-home care placement. Children and and young people who foster are the birth children of foster carers. They may be similarly aged as the child who is fostered and share parental care with the fostered child. Through the role they play supporting their parents and the fostered child, children and young people who foster are thought to benefit in the development of their character via the role.
Children who foster may be adults with their own children who share their grandparents with the fostered child. As adults, they may also support their parents in the fostering role.
Children and young people who foster have also been referred to as “forgotten children”, in consideration of their experience. Children and young people who foster can feel as though their own needs are less pressing, or even less important than those of the fostered child. Wellbeing is threatened and relationships are strained, leading to a decision to end the placement for the fostered child in many instances.
The end of the placement has potential negative impacts for children and young people who foster. Among dependent children of the foster carers, the end of the placement may result in insecurity about the continuity of love and care. Teenage and adult children may experience shame and guilt about the placement ending.
The foster parents, themselves, are likely to be impacted by the placement not working out. Feelings of failure may compromise their caregiving capacity and wellbeing, at least for a time.
For the sake of children and young people who are in-need of out-of-home care, child welfare authorities and fostering agencies need to recognise the role children and young people who foster have to play in placement outcomes, and ensure that they feel important and supported too.
Below are some lines I wrote for children and young people who foster.
I am a child who fosters, but I am not a child.
Only mum and dad think of me that way.
They look after children who cannot live at home.
I thought it would be great at first; someone else to talk to and do things with.
Someone we could help to know what normal family life is.
It started OK.
Now, I feel like I have to fight to be noticed.
Sometimes I feel like the forgotten child.
Mum and dad spend all of their time talking about and responding to the child.
I can see that the child knows it too.
They smile at me whenever mum or dad does something for them.
Like I am the competition in some game they are playing.
And they’re still not satisfied. They want more and more. They have to win.
They get into my things as well. Nothing’s off-limits to them.
Mum and dad don’t even punish them!
They say the child does it because their needs weren’t met at home;
That their parents had problems that got in the way of caring for the child.
That they need consistent care from accessible, responsive, and emotionally-connected adults.
That they need adults who understand them and respond to their experience.
Well, I still need that too.
I need my mum and dad to be there for me without me having to ask; to say the words that show that they understand what is happening for me and our family right now; to show that my needs are important without me having to explain them; and to sit with me and experience what I am feeling.
I need care too.
I want to help my parents, and the child.
I am not a bad person.
It just needs to be fair.
By Colby Pearce
I am a practising Clinical Psychologist with twenty-seven years’ experience working with children and young people recovering from abuse and neglect, and those who care for and have a caring concern for them. I am also an author and educator in trauma-informed, therapeutic caregiving. My programs are implemented in Australia and Ireland, and I am well-known for offering practical and accessible guidance for caregivers and professionals alike.
Disclaimer: While great care is taken to ensure that the advice on this site is widely applicable and based on sound psychological science, it may not suit the individual circumstances of all visitors. If you have any concerns about applicability to your circumstances, please consult a qualified professional near to you.
Join 5,452 other subscribers
Colby Pearce
Search this site
Supporting consistent Therapeutic Caregiving
Companion App for Therapeutic Classrooms and alignment with home.