Borrowing from ideas underpinning culturally safety in service provision, where a distinction exists between being culturally aware, culturally responsive, and culturally safe, there is worth in distinguishing what is trauma-informed practice, as opposed to trauma aware and responsive.
Culturally safe practice involves being culturally aware and culturally responsive, But it is more than this. Being culturally safe includes being sensitive to, and reflective upon, the experience of a cultural group, and developing relationships with that group and individuals within it that acknowledge their experience. It also involves taking action that responds to the experience of the group and individuals within it. Culturally safe practice is distinguished by the emphasis on relationship and acting in consideration of the experience of cultural groups.
Safe practice is relational.
It is worth noting that it is possible to be culturally aware and/or culturally responsive, but not be culturally safe.
Similarly, when working in the area of trauma, it is possible to be trauma aware (this is what you know about trauma), trauma responsive (this is, what you do based on what you know about trauma), and/or trauma-informed. Trauma-informed practice might be thought of as intentional practice where we draw on what we know about trauma and practices that help, but use that to meaningfully connect with the individual or group with whom we are delivering a service and to respond to their experience.
Fundamentally, trauma-informed practice is relational.
As with working with cultural groups, it is possible to be trauma aware and trauma responsive, without being trauma-informed. The necessary additional ingredients are relationships and relational responsiveness.
This represents the cornerstone of success in trauma work; providing a safe and containing relationship for therapeutic work to occur in.
In the absence of relationship, a service cannot rightly refer to itself as trauma-informed.
I have been considering these ideas for a little while and am happy to receive and consider your thoughts. Best wishes. Colby
This morning I read an interesting narrative review of fifteen evaluation studies of trauma-informed care training for foster and adoptive parents (and kinship carers):
Lotty, M, Bantry-White, E, & Dunn-Galvin, A, (2021) Trauma-informed care psychoeducational group-based interventions for foster carers and adoptive parents: A narrative review. Adoption and Fostering, 45(2), 191-214
The review drew the following conclusions:
that there is evidence for the effectiveness of trauma-informed training for those who care for children and young people who are recovering from a tough start to life (albeit, the evidence in the studies they reviewed was mixed);
that effective trauma-informed training incorporates psychoeducation, reflective engagement, and skills building;
that the success of trauma-informed training for carers is likely to be enhanced by parallel practitioner training (eg child welfare staff, schools);
that kinship carers have different (training) support needs; and
that there is a need for more evaluation of training initiatives in this area.
While reading the review I felt both validated and frustrated. Validated, that my own training programs (The (Kinship) CARE Curriculum and The Triple-A Model of Therapeutic Care) are consistent with the conclusions drawn by these authors about what makes for effective and valued training initiatives in this space. Frustrated by difficulties that exist in conducting formal evaluation studies in this area, including for my own programs, including:
The Triple-A Model of Therapeutic Care Implementation in the TUSLA Fostering Service, Donegal, Ireland (ongoing);
The Kinship CARE Project, a two-year project delivered to statutory kinship carers in South Australia (2018-2020); and
Martinthi, an ongoing project to deliver trauma-informed training in an Aboriginal Kinship Care support program in South Australia.
My frustration arises as in all of my training endeavours I do have a parallel evaluation methodology, but lack the time and resources to collate the data we have into articles for publication. I am a sole practitioner with significant psychotherapy commitments and I often joke that I am more a therapist than a trainer when delivering my programs. I have also had the experience that evaluation data demonstrating the effectiveness and worth of training endeavours not being sufficient to ensure its continued support.
In any event, I am pleased to say that I am about to embark on a two-year implementation project in an independent school supporting trauma-informed practice, and that there are plans to conduct a formal evaluation of the intervention. The project will involve the delivery of trauma informed training and support, following a methodology recommended in the article above, reflecting my existing program for schools (Connected Classrooms), which has has been implemented in South Australia and by my trained trainers in Ireland.
It is the case that I have been fortunate to able to develop and implement content and programs consistent with the conclusions above. Both the Triple-A Model of Therapeutic Care and the (Kinship) CARE Curriculum incorporate psychoeducation, reflective engagement, and skills building, parallel training and mentoring for support professionals, and a complementary training program for educators/schools. There are separate curricula for foster and kinship carers, recognising their similarities and their different needs. There is a new curricula that recognises the particular needs of Australian Aboriginal children and their kinship carers.
Relational trauma, such as that which occurs as a result of abuse and neglect, impacts three key areas of relational connection:
The relational connection a child has with others, including those who care for them;
The relational connection the child has with their own self; and
The relational connection the child has with their community.
Where relational trauma has occurred, relational connection with others tend to be weak or superficial, easily replaced, and characterised by mistrust and/or uncertainty about safety and dependability. Similarly, relational connection with self tends to be weak, unstable, and characterised by mistrust and/or uncertainty about worthiness and competency. Further, relational connection with community tends to be characterised by an absence of identification and sense of belongingness with.
These impacts have a range of lasting, further impacts for the development and wellbeing of the child, and their approach to life and relationships. Among these, it leaves them vulnerable to poorly regulated behaviour, wherein such behaviour reflects a lack of concern for the impact of their behaviour on themselves, others, and their community. In time, such behaviours extend to antisocial, self-sabotaging, and self-destructive behaviours.
They act with an apparent lack of concern for themselves, for their relationships, and for the community in which they live.
When we sanction children and young people who are recovering from relational trauma for their behaviour and do little to address the reason for it, we compound their feelings of unworthiness and isolation. We leave them vulnerable to orienting to similar others for relational connection, whereupon their antisocial, self-sabotaging, and self-destructive behaviours become normalised and justified.
Therapeutic work with children and young people who have experienced relational trauma necessarily involves the promotion of strong, functional relational connections with those who care for them, with their own self, and with their community. This is best achieved by approaching their care, management, and psychotherapeutic endeavours in such a way:
that they experience others as sensitive and interested in what is happening for them and why they approach life and relationships in the way that they do;
that they experience themselves as worthy and competent; and
that they experience their community as welcoming and accepting.
Put another way, all therapeutic endeavour with children and young people recovering from relational trauma must facilitate experiences of the following:
My experience is real!
You get it!
I am a person of worth!
I can trust and depend on you!
What a relief!
The world just became a little less overwhelming!
In the passage of time, these experiences support regulating relational connections, where one of the primary drivers for their behaviour is their concern for their own self, their relationship with the important people in their life, and their relationship with the community from whom they experience belongingness.
Relationships regulate! They also support a functional approach to life and relationships. In this sense, regulating relational connections, as described herein, are also reparative relationships.
In order for these relationships to occur, children and young people recovering from relational trauma need opportunity to develop regulating relational connections. This means that they need stability of care in arrangements and communities that support experiences of their worth, competency, and belongingness. Their carers and communities need support to better understand these young people and provide care that strengthens regulating relational connection. This is the primary consideration for those involved in the care and management of children and young people who are recovering from relational trauma, and the primary area of endeavour upon which the success of all other endeavours rest.
Further Reading
For an extended commentary about the use of behaviour management among children and young people recovering from relational trauma, written by international consultant in therapeutic residential childcare and therapeutic services for traumatized children, Patrick Tomlinson, click here.
Schools play a vital role in helping children and young people to recover from a tough start to life, and thrive. My Connected Classrooms programme has been successfully delivered in South Australia, with more than 99% of participant ratings reflecting that the content was informative, practical, and useful, and that they would recommend the programme to other schools.
Connected Classrooms is also delivered in Donegal, Ireland, by my trained trainers in the TUSLA (Child and Family Agency) Fostering Service.
Here is a sneak peak of the content.
To find out more, and to discuss an implementation, contact me at:
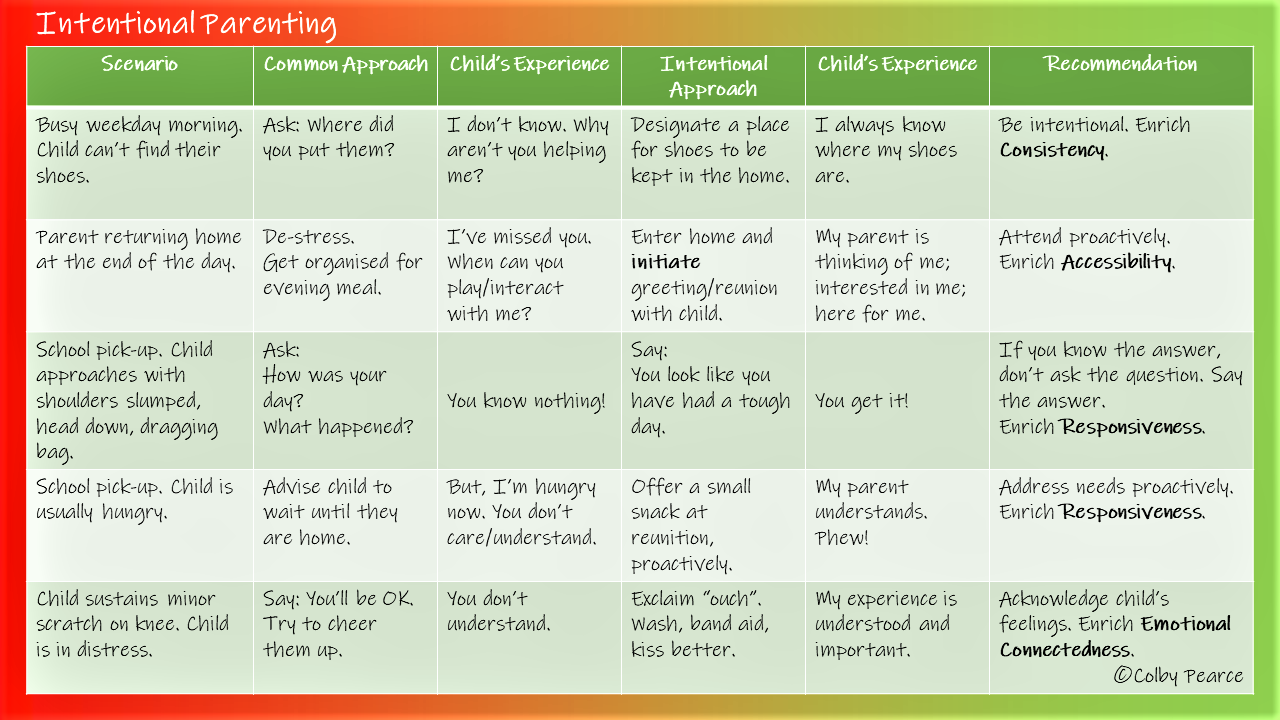
With lots of things that command our attention these days, it is natural to approach aspects of our life and roles in the easiest manner possible. In Psychology, automaticity is concept used to describe times in which we perform a task almost unthinkingly, as if on auto-pilot, freeing up space to respond to other matters. An example most people identify with is the experience of arriving by car at your destination and having little conscious memory of the journey. It can be troubling, though it is natural. Aspects of parenting can become “automatic” too. Children benefit from their parents approaching the role consciously and intentionally. The challenge is to do so without adding to the sensation of overwhelm that is an ever-present risk in modern life. In the CARE Curriculum I put forward simple (and conventional) ways of parenting intentionally that have maximum impact on children, without being overwhelming (for parent or child). I have included some examples in the graphic below.
In the Kinship CARE Project, our outcome data revealed that carers felt more confident in the role and observed improved relationships in the home after completing training in the CARE Curriculum.
For more information about the CARE Model and Curriculum, see:
The CARE Model (Pearce, 2016) offers an evidence-informed conceptual framework for understanding the impact of relationships on the developing person. CARE stands for:
Consistency
Accessibility
Responsiveness
Emotional Connectedness
The CARE Curriculum offers a comprehensive approach to the delivery of culturally-sensitive, trauma-informed and -responsive services among families recovering from adverse life and family circumstances, via the delivery of enriched CARE.
Developmental growth is a central feature of the CARE Curriculum. Key outcomes include:
Growing a consistent, strengths-based and relationship-focused organisational approach to service delivery;
Growing confident and knowledgeable professionals who exhibit key competencies in their practice that support growth in their clients; and
Growth in parental growth capacity to provide consistent, enriched, and reparative care to their young ones.
Personal growth is mediated by individual factors that influence approach to life, relationships, and roles. Key individual factors include:
The beliefs one holds about ourselves, others, and the world (also known as Attachment Representations, Internal Working Models, and Schema);
Central Nervous System activation (also known as Arousal, and implicated in performance and wellbeing); and
Life learning, especially about access to needs provision.
This is the Triple-A Model (Pearce, 2016; 2011, 2010), and represents a framework for understanding how CARE influences individual outcomes. An optimal approach to life, relationships and roles is enhanced through strengthening the influence of:
Secure Attachment Representations;
Optimal Arousal for performance and wellbeing; and
Trust in Accessibility to needs provision.
CARE directly influences Attachment, Arousal, and Accessibility (Pearce, 2016). CARE develops people, thereby addressing the factors that underly common manifestations of psychological impairment, including substance abuse issues, mental health issues, and maladaptive relationships. The CARE curriculum offers an approach to developing optimal functioning and growth via a comprehensive approach to service delivery.
The CARE Curriculum recognises that not all circumstances are the same. As such, there is a particular focus on reflective capacity and practice. Participant organisations, practitioners and parents are supported to develop their knowledge and understanding of the importance of CARE, but they are also supported to reflect on how they can offer enriched care in their work and roles.
A common statement in feedback from practitioners about the CARE Curriculum is that it not only helped them to be better at their work roles, it helped them to be better in their personal roles and relationships. The CARE Curriculum offers the opportunity for people to be the best version of themselves.
Recent and ongoing projects utilising the CARE Curriculum include:
The implementation of the Triple-A Model of Therapeutic Care (a programme of the CARE Curriculum) in the TUSLA (Child and Family Agency) Fostering service in Donegal, Ireland – ongoing since 2016. (Nb. Ongoing implementation maintained by twelve trained local trainers in Ireland).
Martinthi – Aboriginal Kinship CARE Program (A collaboration of InComPro, Bookyana, UCWB, and Secure Start®) – ongoing
Trauma-Informed Psychotherapy – A Programme delivered to Connecting Families with grant support from the DHS Trauma Responsiveness Grant, 2020
The Kinship CARE Project (A Collaboration of The Department for Child Protection and Secure Start®, 2018-2020)
Supporting Trauma Informed Practice in Schools – Programme delivered in DECD regional school and purchased for roll-out in schools in Donegal, Ireland.
The CARE Model, as described in A Short Introduction to Attachment and Attachment Disorder – Second Edition (Pearce, 2016) remains recommended reading for all prospective psychology registrants in Australia who must sit the National Psychology Examination. The Triple-A Model of Therapeutic Care (a programme of the CARE Curriculum) has been favourably referenced in Inspection reports of the TUSLA Fostering Service in Donegal, Ireland, in 2016 and 2018 by the independent inspection authority for health and social care services in Ireland (HIQA).
Some Stats:
A two-year joint-initiative of Secure Start® and the Department for Child Protection (DCP) in South Australia, the CARE Curriculum was delivered to 250 kinship carers across 7 regional and 17 metropolitan locations. Twelve percent (12%) of participants identified as being of Australian Aboriginal descent. Eighty-four percent (84%) of participant kinship carers who completed the training and a three-month follow up survey reported that they were experiencing improved relationships with the children in their care, eighty-nine percent (89%) reported that they felt more confident in the role, ninety-eight percent (98%) reported that they had learnt strategies that had helped them in the kinship role, and one-hundred percent (100%) reported that they had received helpful information. Session by session evaluations showed that more than 98% of participant kinship carers indicated that the training was informative, practical and useful, that they were satisfied with the training, and that they would recommend it to other kinship carers. Analysis of pre-post questionnaires for the first twelve implementation groups identified that kinship carers were more than twice as likely to refer to behaviour being an expression of needs, as opposed to naughtiness, after four training sessions.
References:
Pearce, C.M. (2016) A Short Introduction to Attachment and Attachment Disorder (Second Edition).London, Jessica Kingsley Publishers
Pearce, C & Gibson, J (2016), A Preliminary Evaluation of the Triple-A Model of Therapeutic Care, Foster, 2, 95-104
Pearce, C.M. (2011). A Short Introduction to Promoting Resilience in Children. London, Jessica Kingsley Publishers
Pearce, C.M. (2010). An Integration of Theory, Science and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children – A Triple A Approach. Educational and Child Psychology (Special Issue on Attachment), 27 (3): 73-86
Our approach to life, roles, and relatedness (engagement) is influenced by many factors. Chief among these is the relationships we have with significant others, especially during our developing years. It sounds trite to observe, but our relationships play a key role in our engagement.
The relationships we form toward significant people in our life, and upon whom we depend for care and protection, are our attachments. Our most active period of developing attachments is during childhood, when we form attachments to our parents/caregivers, and also to relatives, siblings, and other significant adults who have continuity and consistency in our life and provide some level of care and protection.
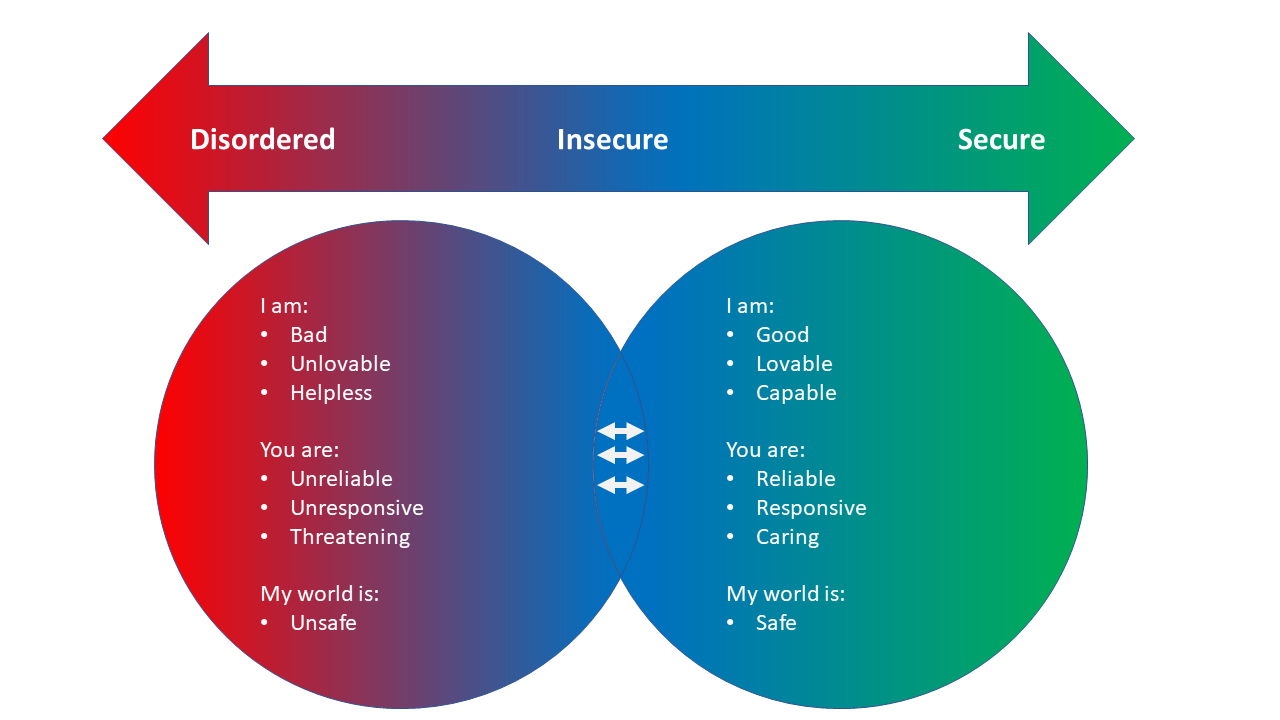
Our attachments to significant others vary, depending on our experience of care and protection from them. Some attachments are secure, meaning that we can confidently explore our world and take on challenges, secure in the knowledge that we have someone we can turn to when we need them; someone who will help us to feel better quickly so we can brave the world again. Other attachments are insecure, leaving us unsure about our access to the support we need to take on the world with confidence after it challenges us in some way. Other attachments are particularly problematic (disordered), as the person we rely on for care and protection is also a source of fear and distress. This type of attachment (also known as Disorganised) is rare and typically only occurs where there has been abuse and/or neglect.
Although some of these attachments are more influential than others (typically referred to a primary attachments), our overall attachment style is influenced by our experience of relationships with all of the people towards whom we have developed an attachment. That is, if we think of attachment as a spectrum that ranges from disorder to security (see below), where each of us sits on the the spectrum is influenced to a greater or lesser degree by our collective attachment relationships.
In consideration of this, we see the positive influence of secure primary attachments and the disruptive (and, at times, destructive) influence of disordered ones. This is brought into further focus when we consider the relationship between where we sit on this spectrum and the the beliefs that form about ourselves, others and our world that develop from our experiences of attachment and influence our approach to life, roles, and relatedness:
Adapted from: Pearce, C (2016) A Short Introduction to Attachment and Attachment Disorder (Second Edition). London: Jessica Kingsley Publishers
All attachments are significant. All influence our approach to life, roles and relatedness. This is particularly important in child welfare and related endeavours where the focus is facilitating recovery from a tough start to life and traumatic relationships, including through the promotion of attachment security. Where the opportunity exists to do so, we need to support repair in disordered attachments and strengthen new attachments through high quality family contact (best connections) and therapeutic child care. It is in the child’s best interests that all attachments are strengthened when attachment security is the goal.
Food for thought:
No matter that you consider the child in your care already has a secure attachment to you, where that child has had disruptive attachment experiences you will need to do more to compensate for the impact of those disordered attachments.
Where possible, our focus must be on repairing attachments that have gone awry. Where this is not possible, all other significant adults in the life of the child will need to do more to support attachment security.
Dear followers of this blog. Just a quick update to let you know that I am collaborating with InComPro Aboriginal Association, Bookyana Cultural and Community Services, and Uniting Care Wesley Bowden (UCWB) in delivering culturally-sensitive, trauma-informed and -responsive support to Aboriginal Kinship Carers in South Australia – Martinthi.
In the language of the original inhabitants of the Adelaide region, Martinthi means ‘to embrace/to clasp/to hold’ and reflects the importance of connection and community amongst Aboriginal peoples.
To find out more about Martinthi, including about accessing support for kinship carers of Aboriginal children placed by the Department for Child Protection, contact 84482881.
To find out more about Secure Start’s endeavours in support of kinship care, visit the website here.
Children and young people who are recovering from a tough start to life are at-risk of experiencing their world as unpredictable and unsafe, and themselves as powerless and vulnerable. Often, they compensate for these experiences by seeking control and influence however they can. Too often, this can be self-defeating and result in sanctions for their behaviour, in turn perpetuating it.
Noncompliance is a strategy these children and young people use to feel as though they can influence what happens to them and feel safe. Any measure to address issues with compliance needs to recognise this and balance it with the need to support feelings of safety and potency (that is, feeling able to influence their world) for the child.
What follows are some gentle strategies that, when used in combination, help to restore adult authority and influence (which children need) while also supporting the child or young person’s feelings of safety and potency. That is, they address the reason for the behaviour, as well as the behaviour.
1. Use ‘controlled choices’
Also referred to as ‘forced choices’, this involves offering the child options that are determined by the adult. The child may be offered the choice of one shirt or another, or between brushing their teeth or their hair first, or between holding the left hand or the right hand before crossing the road. The most important thing here is that the child feels as though they have some say, which meets their need to feel in control and able to influence what happens to them. Nevertheless, adult authority and influence is reinforced as the adult determines what the options are. No choice is too trivial, though the adult must always be happy with whatever the child chooses.
2. Teach a new skill
Children often love to learn a new activity or skill in line with their needs and/or interests. When an adult supports this by teaching them a new activity or interest, the child is motivated to attend to and comply with adult directions. It is intended that the experience of complying is non-threatening, and that the child relinquishes control with no associated negative outcome that threatens their sense of safety and wellbeing. Examples of activities to teach the child include cooking, gardening, craftwork, or board and card games.
3. Don’t ask; say!
Some children pay very close attention to the way we speak to them, including the language we use and tone of voice. When we ask them to do something some children think we are offering them a choice. Rather, gently, but firmly, say what you require the child to do in a manner that projects an expectation of compliance. This strategy, though it may not always result in compliance, helps reduce the child’s perception of being unfairly treated when, having been asked to do something and exercising their perceived choice to say no, the adult insists they comply anyway.
4. Help them be compliant
When you direct a child to do something, help them to be compliant. Do part of the task. The intent here is for the child to experience the adult as accessible, supportive, and safe when compliance is expected.
5. Catch them in the act
This is potentially the most helpful strategy of all. What I mean here is to observe the child and what they are doing, and gently direct them to do the very same activity. This is intended to help them get used to following directions, with nothing bad happening, and support a perception of adults being in control whilst avoiding challenging their own sense of choice. Again, nothing is too trivial to direct the child over. The only caveat is that it must be an activity that the adult is fine for the child to be engaging in. After a while, you may also be able to anticipate the child’s next move and direct them to do this too.
Watch this playlist to see how these strategies can be implemented in a way that supports adults being in charge without making ‘Bella’ feel unsafe:
Below is a statement that reflects the third ‘A’ in the Triple-A Model – Accessibility (to needs provision). It captures my thoughts and my response when I am talking to caregivers about their experience of the behaviour of a child who is recovering from a tough start to life. Embedded in this response is the notion that children do not do anything for no reason. If we can hold on to this idea, we might then ask ourselves what is going on for the child? This is the first step in the process of making and maintaining a relational connection with the child that, ultimately, represents our best chance of being a positive regulating influence over their approach to life and relationships. Often, the behaviour of the child who is recovering from a tough start to life reflects their preoccupation with a need that was met inconsistently during the developmental period, and their endeavour to reassure themselves about access to needs provision. Responding to the need facilitates for the child the experience that their need is understood and important, that it matters, that they matter, and they can rely on you for needs provision. This is a relief for the child, thereby supporting lower arousal and reduced vulnerability to anxiety and additional behaviours of concern associated with activation of the fight-flight-freeze response. It supports functional learning about access to needs provision a reciprocal connection from the child.
The statement goes like this:
Children are not preoccupied with physical, emotional, and relational needs that were met consistently during the (early) developmental period. They are preoccupied with needs that were met inconsistently. Their behaviour, in turn, reflects their preoccupation. To address preoccupied behaviour, we must first meet the need that gave rise to the preoccupation.
Disclaimer: While great care is taken to ensure that the advice on this site is widely applicable and based on sound psychological science, it may not suit the individual circumstances of all visitors. If you have any concerns about applicability to your circumstances, please consult a qualified professional near to you.
Join 5,452 other subscribers
Colby Pearce
Search this site
Supporting consistent Therapeutic Caregiving
Companion App for Therapeutic Classrooms and alignment with home.